
Hell o from the 32nd congress of ECTRIMS, & the 21st conference of Rehabilitation in MS.
o from the 32nd congress of ECTRIMS, & the 21st conference of Rehabilitation in MS.
ECTRIMS is ‘ Europe’s and the world’s largest professional organisation dedicated to the understanding and treatment of multiple scelrosis’
With over 8000 delegates, all specialising, of with a special interest, in MS, it’s a privilege to attend! Loads of lectures run concurrently, so you can never attend everything. And the really science-y lectures, that are not yet going to make a practical difference to my patients, tend to go over my head a bit. Or a lot, depending! So here’s a digest of what I’ve learned so far, that has a practical application for people with MS!
The intro – X. Montalban (Spain)
Good to hear the current aims:
- Evolving the Diagnosis of MS, so it can be made more quickly, but still be accurate. ( did you know there are 100 other conditions that can cause MS -like symptoms?)
- getting better at Prognosis – working out who is likely to develop definite MS, and who with MS is most at risk of becoming disabled
- in order to Personalise treatment – this means ” the right drug, at the right time, for the right person. And, at the right price.” Moving away from ‘first-line’ and ‘second-line’ treatments, to personalised treatments. Did you know that people treated with a disease modifying treatment before the second relapse developed less disability?
This leads into a presentation I saw in the break:
Brain Health – G. Giovanonni (UK)
This is a campaign led by Gavin Giovanonni of Bart’s ( UCL) hospital, London, and an international steering group of MS experts, with funding from some of the major disease modifying therapy (DMT) manufacturers.
The focus was on healthcare professionals, to improve services for people with MS, with, again, speedier diagnosis, prompt treatment, adequate follow up to find out if treatment is working, to allow an alternative or more aggressive treatment if the original one is not having a good enough effect, and certain standards of MS care – eg – noone with MS should get a pressure sore in your area of care etc.
People with MS can get involved with this project, and download the guide to help get what you need from your neuro services. It also strongly recommends the lifestyle measures to keep your brain healthy that have the most robust clinical evidence in MS to satisfy the health service, like:
- Exercise

- not smoking
- not being oeverweight
- not using too much alchohol
- exercising your brain
- continuing with prescribed medical treatment
You know that I believe in doing even more!
Rehabilitation strategies – what works? – J. Freeman (UK)
 This presentation was kind of frustrating. Only because we all know physios, OTs, psychologists, physical therapists who do great work that makes a big difference to people with MS’s health and lives. But because we’re not organised or funded to perform large scale randomised controlled trials ( as drugs are), most of the studies done aren’t ‘robust’ enough to prove the effects. This is a problem in and with the evidence based medicine approach – it has a tendency to turn all medicine into pharmaceutical medicine.
This presentation was kind of frustrating. Only because we all know physios, OTs, psychologists, physical therapists who do great work that makes a big difference to people with MS’s health and lives. But because we’re not organised or funded to perform large scale randomised controlled trials ( as drugs are), most of the studies done aren’t ‘robust’ enough to prove the effects. This is a problem in and with the evidence based medicine approach – it has a tendency to turn all medicine into pharmaceutical medicine.
The interventions whose evidence is robust enough are:
- Exercise ( this is coming up time and time again! Did you know that exercise has recently been found to be not just good for you in all the ways we already know, but actively anti-inflammatory?)
- Endurance training, and
- Supported treadmill walking ( probably not massively better than other interventions, just done good research, possibly due to industry funding)
Improving mobility – D. Centonze ( Italy)
An extremely scientific presentation, suggesting that mobility could be preserved by measures that help to restore excitability to the nerve connections; ‘long term potentation’ and ‘synaptic plasticity’
At this point I really wished that the organisers would round up their presenters and give them presentation skills; however, what I THINK he said was:
Certain interventions can restore excitability, and thus improve mobility. And these are:
- Exercise ( yes, exercise again!)
- SSRI antidepressants (I’d have to know a lot more about that before recommending this. Like, is this all theoretical or have they conducted studies to show this effect??
- Cannabinoids (Likewise)
- or drugs that use these pathways for their effect
- Electrical stimulation (because it activates cannabinoid and dopamine receptors)
- And disease modifying therapy, because it helps to prevent inflammation, which is harmful
Treating MS bladder dysfunction – J. Panicker (UK)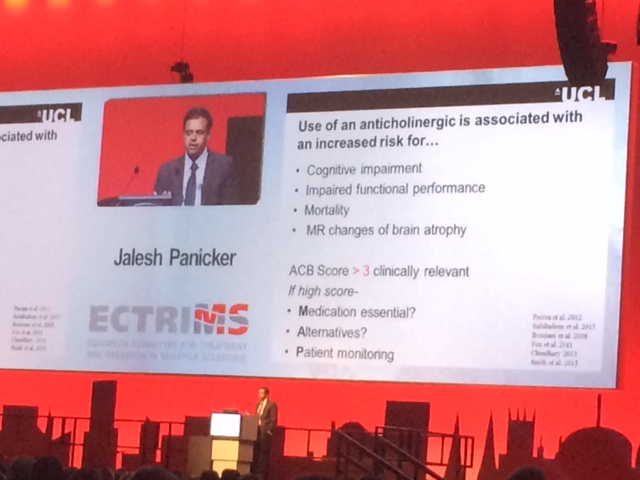
Nothing new for me as an MS Nurse here; I’ll do a blog on the bladder; but confirmed the point I made earlier in this post about alternatives to anticholinergics that cause cognitive problems, and nice to see it being discussed. Add to that: Darifenacin or Tropsium if you can’t get Mirabegron.
Chasing the driver of fatigue in MS – V.Biberacher (Denmark)
Now this was really interesting. Why people get such fatigue in MS has always been a big question, and one that there are a lot of theories about. These investigators wanted to see
whether it was more associated with damage and lesion load in the brain, which can be measured by MRI scanning, or by inflammation, which can be measured by inflammatory markers in the cerebrospinal fluid ( CSF ) taken by lumbar puncture.
What they found, was that there was no significant relationship between damage and lesion load in the brain, but there was a significant relationship between inflammatory markers in the CSF. This suggests that inflammation, rather than structural damage, is responsible for fatigue in MS.
The take-home from this is that there are many ways to help reduce inflammation in your body – both your drug treatment, and lifestyle measures – eating an anti-inflammatory diet, getting good rest and sleep, becoming more resilient to stress, exercising, sunshine, vitamin D…
Dual lead deep brain stimulation for tremor – S. Oliveria (USA)
Study showing good effects on refractory ( ie won’t respond to any treatment/ drugs) tremor, in a small group of 11 people. 8 (73%) showed benefit at 6 months. 2 did not benefit; they had ataxia ( like clumsiness) rather than tremor. One got infected and had to have the leads removed. Kind of let down by the fact that they used a scale to show effectiveness, which didn’t show the actual result for the person’s functional improvement. So worth finding out about, but not a sure thing until we hear what the results of treatment for the actual people were. Grr!
Hot topic – bone marrow transplantation is a justifiable treatment for active relapsing remitting MS
Now I’m getting too hungry to report on this debate about stem cell /bone marrow
When you want to be in two places at once….
But I’ll try to finish this off tomorrow!
All the very best!
Miranda

Great BLOG Miranda and look forward to catching up tomorrow.
Little puzzled by the bit on “Chasing the driver of fatigue in MS” since I’d say fatigue was a big thing for me, yet I have lesions but my Neurologist found no inflammation in the Lumbar Puncture. However, my Oxygen Therapy really improves my fatigue levels, and that’s supposed to be because it feeds Oxygen through to the lesions in the brain? Strange, but then we are all different.
Thankyou! Ah well he would have been looking for Oligoclonal bands at that time; whereas anylising lots of other stuff can find other inflammatory markers. However, nothing’s cut and dried in MS, we also know that destruction of the myelin sheath means that people with MS expend far more ATP to send messages than people in normal health – maybe I should add that point! Interesting point about HB02, and I always state that many people find it helpful in my info about fatigue for patients. See you at MS LIfe!