Wow, what a full on 3 days for the brain! So inspiring to see a sea of research posters, a vast menu of presentations , and 8000 engaged delegates filling up on the latest research.
Bone marrow transplantation ( HSCT/stem cell) – is it a viable treatment for active relapsing remitting MS – debate
Consensus was: safety is improving – from 2011 the mortality rate has been 0.3% rather than 1-2%. Due to impressive rates of NEDA ( no evidence of disease activity – relapses or on MRI) – 80% at 2 years and 70% at 4 years in one study;
Yes, but ONLY in cases of early/new, highly active/aggressive relapsing remitting MS, where person is young, still walking, and treatment with first & second line treatment have failed.
And now for something completely different, and please DO try this at home(!): Seriously, I will be
Lipoic acid for neuroprotection in secondary progressive multiple sclerosis: results of a randomised placebo-controlled pilot trial – R.I. Spain (Portland, United States) 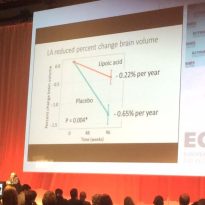
This beautifully carried out RCT had people with progressive forms of MS taking 1,200mg of Lipoic Acid, a supplement often sold as an ‘anti-oxidant’, and also called ‘alpha-lipoic acid’ once a day. A control group took a placebo.
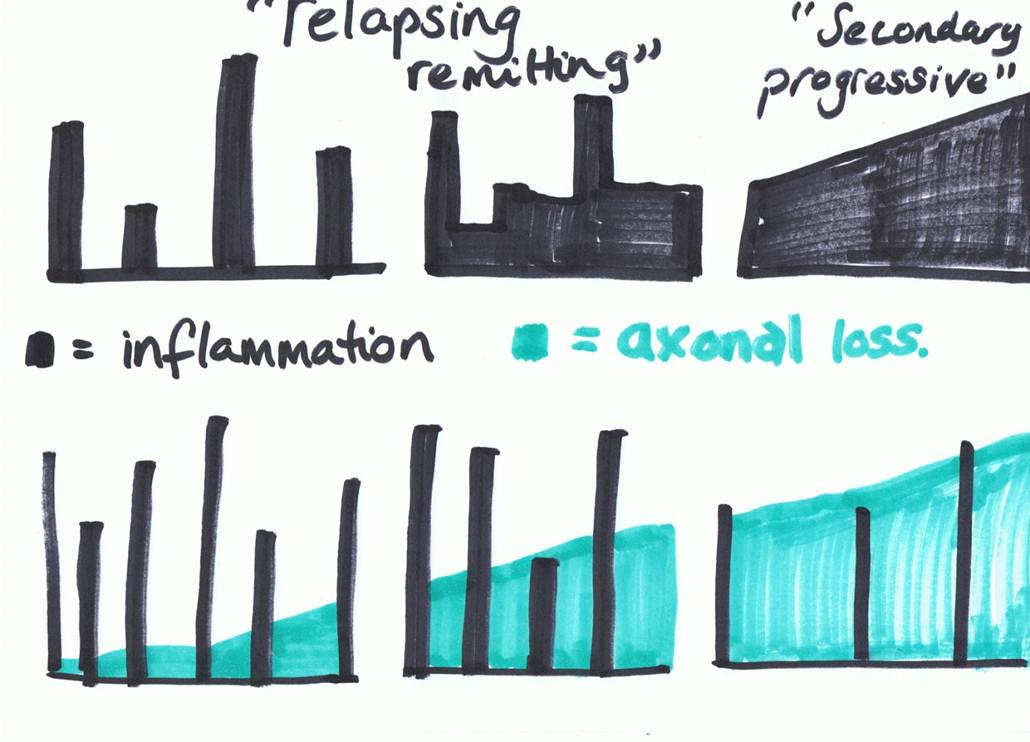
After 2 years, the group taking the lipoic acid had a whopping 66% less brain atrophy on MRI scan ( showing less loss of brain cells), taking them back to a normal rate of brain atrophy, and half the number of falls.
Love it when something so harmless is investigated properly and found effective. Especially good to have something positive for progressive MS!
Comparison of Beta Interferons, Fingolimon, Alemtuzemab (Lemtrada) and Natalizumab ( Tysabri)
showed that as we know, effectiveness in reducing relapses from lowest up goes: Interferons, then Fingolimod, then Alemtuzemab and Tysabri. The last 2 showed the same effectiveness in preventing relapses. Natalizumab also showed improvement in disability in the first year, but not after that. and as we now the side effect profile and the way you take it is very different. Tysabri also has a rebound effect if and when you stop taking it.
Alemtuzemab
research was presented that showed this drug performing very well in ‘resetting’ the immune system. Around 60% of people did not need more than 2 infusions, and NEDA ( no evidence of disease activity) was very high., but only when used EARLY. Time to change from the ‘wait and see’ attitude? This is the push from leading MS experts. Maybe check in with the MS Brain Health campaign if your neurologist is dragging their feet.
Vitamin D 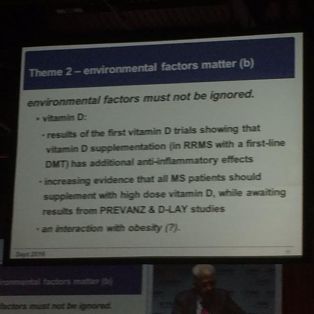
very strong evidence coming through from numerous sources that notwithstanding previous medical controversies and uncertainties, all people with MS should be on high dose from diagnosis – 4-5000 IU daily at least, and testing ( backs up info already posted on this blog) MS Base ( a database with over 41,000 people with MS’s records) showed a clear seasonal peak in relapses around the world, at the end of winter; with a time lag, shorter in colder countries. Low vitamin D levels were the strongest risk for progression in another study, and added a further anti inflammatory effect to people already on a disease modifying treatment, in another.
One study found that people with MS given 100,000 twice a month for 2 years had a 60% reduction in relapse rate, and a 78% reduction in new lesions, compared to placebo. Powerful stuff, hopefully enough to finally swing the doubters.
Siponimod for progressive MS
presented as promising new treatment but I missed that session so – investigate!
Scientific highlights presentation – was split into 3 sections ‘migration and CNS injury’, ‘Gut and Food’ and ‘remyelination and oligodendracytes’
At the end of the event, I was really surprised to see these slides in the highlights – I missed the full presentation but one slide went like this:
 Oxygen
Oxygen
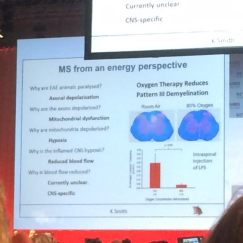
MS from an energy perspective.
Q:Why are animals with experimental animal MS paralysed?
A: Axonal ( nerve) depolarisation ( can’t send messages)
Q Why are axons depolarised?
A: Hypoxia ( lack of oxygen)
Q: Why is the inflamed central nervous system hypoxic?
A: Reduced blood flow
Q Why is blood flow reduced?
A: Currently unclear , CNS specific ( ie we don’t know, but it’s just the central nervous system.)
Went on to describe how animals with this experimental model of MS respond very well to hyperbaric oxygen: Oxygen therapy reduces pattern 3 demyelination.
So maybe we will see some new research showing usefulness of hyperbaric oxygen? If you can access it, I always say that it’s worth trying, and observe the effects on yourself.
Diet and Gut in MS
Feels like finally, the importance of aspects of diet is being addressed and listened to in MS research. In fact all present were enjoined Not to ignore environmental factors. Hurrah! a strike for logical thinking!
This was a feature of quite a lot of research at ECTRIMS. Lots of research on the role of the Biome ( bacteria in the gut) and how it affects MS. Interesting, exciting, but we still haven’t nailed practical application yet, so best bet is Take a daily probiotic capsule or powder, with as many different strains in as possible. And do these things, discussed previously.
Being overweight was identified as a serious risk factor for both developing, and worsening with MS. If you’ve got pounds to lose, check out the excellent ‘Fast Diet/ 5:2 diet’, showcased by Micheal Moseley on the BBC -https://thefastdiet.co.uk/ fasting also has benefits for inflammatory conditions.
Salt:
salt stored in the skin was posed as a driver for auto-immune neuroinflammation in one paper. People with MS were found to have higher levels of salt in the skin….so that too… we could all cut down our salt – most is found in processed foods… and as you do it, your tastebuds acclimatise so it won’t mean you won’t taste your food.
Ending on a high
Conference ended on a high note, celebrating the huge progress that has been made in preventing disability – progress that started even before the availability of the disease modifying drugs, but has in recent years added a further 15 years of non-disabled life to the average MS-er, and is still making leaps and bounds.
I hope I’ve made an accurate summary of the sessions that I attended – mistakes are possible, and they will be all mine. If you spot one, please let me know!
That’s all for now, til the next time!
miranda