OH NOOO! I hate it when a drug that was a useful tool turns out to have really bad side effects!
I hate it when a drug that was a useful tool turns out to have really bad side effects!
In an ideal world, we’d all be drug free, of course, but hey – noone is taking this stuff for fun!
You may have seen in the news recently the reports linking drugs with an anticholinergic effect with dementia and cognitive problems. This type of drug includes over the counter anti-histamines for allergies/hayfever. Many people with MS take anti-cholinergic drugs for bladder overactivity/urgency, which include:
Detrusitol / Tolterodine, Solifenacin / Vesicare, Oxybutnin / Lyrinol XL/Kentera patches, Fesoterodine fumarate / Tovias, or Darifenacin / Emselex
and many take a low dose of tricyclic antidepressants for nerve pain, which include
Amitryptilline, and its less sedating sister, Nortryptilline.
Awareness has been building about the link between anticholinergics and cognitive problems; in fact a review on the subject in 2009 found twenty-seven studies that met their inclusion criteria, of which, all but two found an association between the anticholinergics and either delirium, cognitive impairment or dementia. (1)
This month, however, the a new study on 3434 people provides the ‘strongest evidence yet’ that anticholinergic drugs may increase the risk for dementia in older adults.( 2)
All studies done on the effects of anticholinergics have been done in older adults “There is no data on how these drugs may affect younger people, but I personally will avoid taking anticholinergic agents,” – Shelley Gray, author of the study.
What if you’re only on a low dose?
Unfortunately if that’s a continuous dose, it still counts. Eg 3 years of taking low dose medication with anitcholinergic effect for neuropathic ( nerve) pain counts as high use.
What to do if you’re on one of these meds?
Obviously, full blown dementia in old age is unlikely to be reversible. However, previous studies on people coming off anticholinergics found that the detrimental effects on thinking were reversible(3), so don’t panic!
What are the alternatives?
For the bladder, two of the alternatives I actually mentioned in a recent post: tibial nerve stimulation, and mirabegron, a selective beta3 adrenoceptor agonist, which works in a different way to anticholinergics. NICE has recommended mirabegron as an option for treating overactive bladder (OAB) “only for people in whom antimuscarinic drugs are contraindicated or clinically ineffective, or have unacceptable side effects”, which means that you may have to fight for it, or get the help of your continence service to request it, due to the difficulties these days in accessing medicines that are not the cheapest available.
As you will know, if you have urinary urgency with MS, you should never take medications for it before being seen and scanned by a continence nurse, as the problem can sometimes be cause by the bladder not emptying properly, and in this case, the drugs don’t work, they only make it worse!
If however, you’ve been assessed, and found to have a severely overactive bladder, one option, under urology, is to have botox injected into the bladder wall, which completely relaxes the bladder, and lasts for several months. You have to be willing and able to take on intermittent self catheterisation if necessary, and when it works, it can be a real life changer.
Non drug options?
One of the commonest (? rude?)- most common things that people report are being benefitted by hyperbaric oxygen at the Therapy Centre is bladder urgency.I don’t deal in ‘miracles’ but there’s a link in today’s telegraph online about it: http://www.telegraph.co.uk/lifestyle/11376969/The-miraculous-healing-powers-of-oxygen.html
Other little pieces of magic can be reflexology or acupuncture. Small studies have shown positive effects for treating this problem, and I have had patients reporting good results after seeing our reflexologists, Theresa and Lorna but non are large or robust enough to become very official ( the studies, not Theresa and Lorna! )
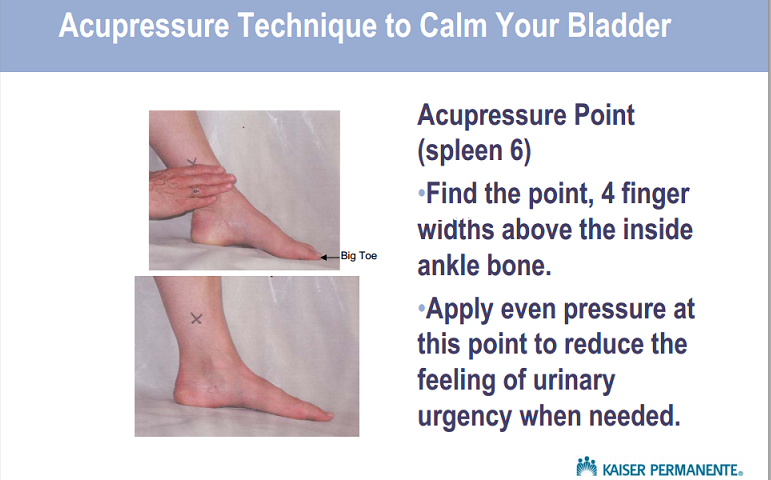
Here’s one of the main acupressure points for self help: 
400-600mg of magnesium can sometimes have a calming enough effect to reduce bladder symptoms, and reducing caffeine and bladder retraining can also have a good effect. (4) Your best source of expertise on the bladder is your continence service nurse, and its a good idea to go back every couple of years to stay one step ahead of any bladder problems in MS.
What about nerve pain?
Luckily, there are other effective medications for distressing neuropathic pain in MS, the most commonly prescribed being Gabapentin, and its updated ( and more expensive) version, Pregabalin. Although there are, as with all drugs, possible side effects, the most common for Gabapentin being weight gain, they are not linked with the dangers to cognition that the anticholinergics are.
At the MS Therapy Centre, we are lucky to be able to offer APS Therapy, which has had a great result for many people, and the therapies Shiatsu and reflexology also have potential to help. So – if you find that you are regularly taking medication with an anticholinergic effect, have a think about the alternatives, and work with your GP to change your prescription, for a clearer head.
1) Clin Interv Aging. 2009; 4: 225–233. Published online 2009 Jun 9. PMCID: PMC2697587
The cognitive impact of anticholinergics: A clinical review
Noll Campbell,
4 Malaz Boustani,
1,2,3 Tony Limbil,
1 Carol Ott,
4,5 Chris Fox,
6,7,8 Ian Maidment,
6,7 Cathy C Schubert,
3Stephanie Munger,
1,2 Donna Fick,
9,10 David Miller,
3 and
Rajesh Gulati11
2)
Cumulative Use of Strong Anticholinergics and Incident DementiaA Prospective Cohort Study
Shelly L. Gray, PharmD, MS1; Melissa L. Anderson, MS2; Sascha Dublin, MD, PhD2,3; Joseph T. Hanlon, PharmD, MS4; Rebecca Hubbard, PhD2,5,6; Rod Walker, MS2; Onchee Yu, MS2; Paul K. Crane, MD, MPH7; Eric B. Larson, MD, MPH2,7
JAMA Intern Med. Published online January 26, 2015. doi:10.1001/jamainternmed.2014.7663
3)
-
Effects of discontinuing anticholinergic treatment on movement disorders, cognition and psychopathology in patients with schizophrenia.
4) Hartmann KE, McPheeters ML, Biller DH, Ward RM et al. Treatment of Overactive Bladder in Women. Evidence Report/Technology Assessment No. 187. Rockville: Agency for Healthcare Research and Quality (AHRQ). August 2009. [Full text] [PubMed]