very proud as one of my heroes, Val, accepts Big Society award for the MS Therapy Centre
Woop woop! My workplace, the Bedford MS Therapy Centre wins Big Society award!
Reply

very proud as one of my heroes, Val, accepts Big Society award for the MS Therapy Centre
Recently we had a local newspaper article that started off so well, about the exciting results we’ve been getting with APS Therapy at the MS Therapy Centre in Bedford. Then in the last paragraph, it said that I was now offering to rent APS machines to MS patients, which made it sound as though I was renting them to my own patients, and was an unintentional mistake by the journalist.

To be clear, people with MS who live in Bedfordshire or Northamptonshire can come to the MS Therapy Centre and have this therapy for free, and I will be involved, as the MS Nurse there.
In my private business, I do a variety of therapies, not aimed at people with MS, and I tend to keep the 2 separate. I have added renting APS Therapy machines to my business, and this is available for anyone from the general public who has pain. I am advertising this in local papers and on my business facebook page.
At the moment, I am the only UK supplier of APS Therapy machines. However, if & when people with MS want to purchase a machine, I supply them direct from the manufacturer, without taking commission, as long as they can prove that they have MS. People who are not members of the Beds & Northants MS Therapy Centre will still need to pay for their training, treatment plan and follow up time. This is important to know, as in June/July there will be a peice in the MS magazine New Pathways about what we are doing at the MS Therapy Centre, and also about my business.
Hope this makes things really clear
If you have Relapsing Remitting MS, with 2 relapses in the past 2 years, and walk without a stick, then it’s important to know about this.
Alemtuzimab, ( called Campath whilst being trialled at Cambridge for many years,) is a powerful immunosupressant, ( like chemotherapy), which is given as an IV infusion, has been shown to be very effective in stopping relapses and disease activity in MS – including progression of disability, as long as it is given before disability sets in.
In a trial of Alemtuzimab reported in 2008, compared to interferon beta-1a, alemtuzumab reduced the risk of sustained disability by 71%. There was also improvement of disability scores in the treatment group. After 36 months the mean disability (EDSS) score in the alemtuzumab group had improved from 1.9 to 1.51 while that of the interferon group worsened from 1.9 to 2.28. After 5 years, those who had had alemtuzimab had 67% less disability, and 72% were relapse free, compared to 41% of the interferon treated group.
This makes it much more effective than the current disease modifying treatments ( DMTs), which can show reduction in relapse rates, but not prevention of progression.
This slide, from Neurologist Joanne Jones, at Addenbrookes, shows the placement of current drugs ( including stem cell treatment) in relation to efficacy ( effectiveness) and safety.
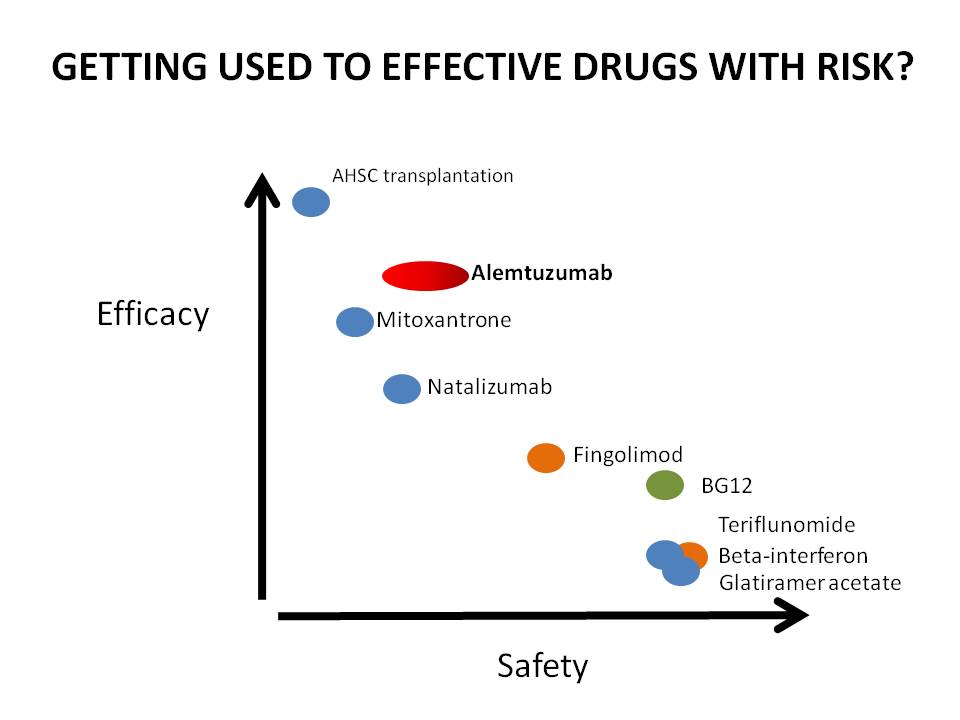 If you can see this, stem cell is at the top on the left, indicating highly effective when it works, but risky. DMTs are at the bottom on the right – safe – but not so effective as the newer agents.
If you can see this, stem cell is at the top on the left, indicating highly effective when it works, but risky. DMTs are at the bottom on the right – safe – but not so effective as the newer agents.
Nataluzimab is the generic name for Tysabri.
It also has more risk of serious side-effects than DMTs, so weighing up your risk of serious disability from MS against risk of contracting rare but serious side-effects, needs to be thought about very carefully.
So what are the risks of treatment? About 30% of people treated with Alemtuzimab get a different auto-immune problem at some point after treatment, and this is generally a thyroid problem, which can be treated. About 1 in 100 develop a blood clotting disorder, ITP, which can be treated if caught, but one person has died. In trials on Alemtuzimab, there was one death from lymphoma which may have been related, and there have been rare but potentially fatal kidney problems.
At present Alemtuzimab is going through the licensing procedure. Once it has been licensed, it may be rationed, and only offered to those who have relapsed on the normal DMTs.
However, the CAMTHY trials, which are testing to see whether a particular drug given with Alemtuzimab can make the treatment safer, are currently open to anyone with MS in the UK who meets the criteria. You need to have RRMS, have had 2 relapses in the past 2 years, be able to walk without a stick, not have Insulin dependent diabetes or thyroid problems, be under 50, and not have had previous immunosupressant drugs ( but DMTs are ok)
Because I’m not involved in the research, and don’t have the time to analyze it thoroughly, I can’t present the risks and benefits any more clearly than this at this point. You can read about the work done so far here: http://www.colescambridge.org.uk/index.htm
and about how to be referred to Addenbrookes to discuss taking part in the trials, here:
http://www.colescambridge.org.uk/trial%20participation.htm, and if you are seriously interested and meet the criteria, you can discuss the pros and cons with one of the doctors running the trial, at Addenbrookes, after referral by your GP or MS Specialist Nurse. It may be worth reminding your GP that there is not a cost to them for this referral or treatment, as the trial has its own funding. Worth very serious thinking about.
I was proud to present this poster at the MS Frontiers conference – Fantastic findings re Flax seed oil – 49% less relapses in people with MS that took it, research by http://www.overcomingms.org just been accepted for publication.. Will post more info asap.
Also coming up – and important to know about if you have RRMS -Campath/alemtuzimab/lemtrada trials
and – interesting stuff from MS Frontiers conference
|
|||||||||||||||||||||||||||||||||||||||||
APS Therapy update; our first results for people with pain

At the MS Therapy Centre, we are trialling a new electrical treatment for pain, called APS Therapy (See previous issues for an explanation!)
Here’s a round-up of our results so far.
Some people have completed a course of treatment, some are ongoing, and some have only just started and had a few sessions. We are working hard to make sure we collect better data in future so we can answer more questions. We used the ‘Visual analogue pain scale’ which measures pain out of 10, with 0 being ‘no pain’ and 10 being ‘the worst possible pain’
Neuropathic pain in limb: 7/10 down to pain free; complete pain relief which lasts 4-5 days, but appears to need long term treatment as comes back after this time.
Neuropathic pain in the feet and feeling ‘like walking on hot sand’, constant, 6-7/10 down to 3-4/10 in 3 weeks, hot sand feeling down to ‘not very often’ and improvement in blue-ish discolouration due to poor circulation..
Hip pain 6/10 constantly, complete relief since the first week, has not returned, and a decrease in neuropathic pain in the leg from 4/10 to 2/10 in 3 weeks.
Back pain, 8-9/10, worse on exercise, down to pain-free, 2-3/10 on exercise. Treated x 2 weekly for 6 weeks. Has not returned, 1 month after end of treatment. Leg pain, ‘pounding, throbbing’, 8/10, down to pain-free, has started to creep back since recent sensory relapse.
Long term shoulder pain, 2-7/10 to ‘much better’ but has since had to stop treatment for personal reasons.
Hip pain 10/10 plus, no benefit. This could be because there’s a serious problem that needs attending to underlying the pain, or because high doses of opiate painkillers make the treatment less effective. We’ll be helping this person get the right investigations and treatment, and maybe try again later.
Arm pain, possibly radiating from shoulder, no cause detected by GP, 2-3/10 with episodes of stabbing pain 5-6 x a week at 10/10; down to 1& half/10, no episodes of stabbing pain after 2 weeks of treatment
Headaches, constant, 7/10 down to pain-free, and back pain 7/10, down to 1/10, plus complete relief from insomnia.
Chronic pelvic pain, 2-4/10 normally, 7-8/10 when bad, happening less frequently, tramadol usage has dropped from daily to 2-3 x a week, now reducing Amitryptilline also.
Hip pain, 8&1/2 /10, very severe, ‘sickening’, no change, although improvements in sleep pattern. We are helping this person get investigations carried out.
Hip pain, 7/10, 8/10 when worst, down to 4/10 after 3 treatments, but also had deep physio manipulation prior to starting!
Severe muscle spasm and spasticity, no change after 12 weeks +
MS fatigue; no change
MS fatigue; no change
Headaches, 4-6/10, 9/10 when worst, 2-3 x a week, for most of life, worse since starting Rebif, down to pain-free; has had one headache since starting therapy, when had not drunk enough water. Has not taken regular painkillers for weeks. Back pain, 4-6/10, 7-8/10 when bad, down to 3/10. Stopped Naproxen and Co-codamol use. Knee pain (which was unreported, as forgot about it) has disappeared. Much more energy, staying up past bedtime, cleaning.
People who’ve just started:
‘Squeezing’ altered sensation feeling, 7/10, 9/10 when worst, no change yet after 4 sessions; muscular pain in shoulder blade area, 4/10, 8/10 when worst, down to 2/10 after 4 sessions.
Shooting, stabbing, intermittent pain in knees, 5-10 -11/10 down to 4/10 max after approx 2 weeks
Tennis elbow, 8/10, worst 10/10, now 6/10, worst 8/10, significantly improved range of motion and no sleep disturbance due to pain, after one week’s treatment ( and also carrying on with Bowen treatment)
So in summary, in our study so far, 18 people have used the APS Therapy at the Centre, 17 with MS and one member of staff. 2 tried APS for fatigue, and 1 for spasticity, and disappointingly, these conditions have not experienced a significant benefit to date.
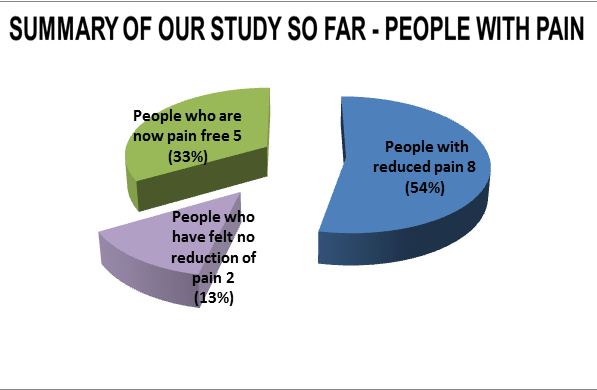
15 people used APS Therapy for pain. Of these, 13 have felt a significant reduction in pain, and 2 have not. 2 also report a significant increase in energy. Of the people with pain, 5 have achieved pain-free. Of these, 2 people’s pain has not come back since completing the course, one needs to maintain therapy once a week, and 2 are still completing their course of treatment.
We’re delighted that Denise, who many of you will know already from the Gym, has now been employed 3 days a week to also help run this project and help people to use the APS machines at the Beds and Northants MS Therapy Centre. If you are having a problem with pain, you can come and see me (Miranda) for a full pain assessment. If APS Therapy seems like an appropriate course of action and you:
a) Can get in 3 x a week ideally; twice if necessary, and
b) Can drink 1&1/2 litres of water a day, and
c) Have none of the following: heart attack, deep vein thrombosis, stroke or pulmonary embolus in the past 3 months, cancer, epilepsy, or pregnancy.
I will refer you on to Denise, to start a 6 week treatment plan. For some pain, APS Therapy may be able to completely and permanently resolve the problem. For some people it may not help at all, and for others, it may significantly reduce or resolve the pain, but need to be continued to keep getting the effect. In those cases we can help you to purchase your own machine direct from the manufacturers if you wish, and also to apply for charitable funding if money is a problem.
It’s very exciting to be working with such a new, drug-free treatment. We intend to start helping people to review their medication once they get a good result, with a view to reducing pain medication.

My Super Nurse winners 2013
OMG!!! So happy today – what a lovely surprise 🙂

The winners of the MS Trust ‘My Super Nurse’ award for 2013 are Miranda Olding of the MS Therapy Centre Beds & Northants and Lindsay Harrison of Salford Royal NHS Foundation Trust.
Since voting opened at the end of January we’ve received hundreds of nominations from people affected by MS, from Derry to Great Yarmouth, from Truro to Dundee. Over one hundred different nurses were nominated: that’s almost half of the entire MS specialist nurse workforce!
Each nomination came with a short tribute to the nurse being nominated, giving a little insight into the tremendous impact they can have.
You can see a small selection of the nominees, and read short interviews with them, on our Super Nurse nominee gallery.
We’d like to thank everyone who took the time to nominate their nurse this year. It’s amazing to hear real-life stories of the difference MS specialist nurses can make, especially at a time when many of them find their funding is under threat.
Due to overwhelming numbers of nominations this year, and the fact that two nurses in particular were so far ahead of the field, we felt it only fair to announce joint winners of the award this year.
So we are very happy to announce that the MS Trust ‘My Super Nurse’ winners for 2103 are Miranda Olding from the MS Therapy Centre Beds and Northants and Lindsay Harrison of Salford Royal NHS Foundation Trust.
You can read an interview with Lindsay here and watch an interview with Miranda here.
“I couldn’t think of a nicer thing to win,” said Miranda on being told she was a Super Nurse. “I’m very grateful to my patients, employers and the MS Trust for such a lovely award (and a great job).”
“To receive an award initiated by the people under my care is probably the highest honour a nurse could achieve,” said Lindsay. “I am so grateful for the lovely feedback and the support of the MS Trust, who work hard to improve the lives of people with MS through information, support and further educational opportunities for nurses.”
At the MS Trust we believe that everyone with MS should have access to a specialist nurse, but we are very aware that there are still gaps in the service. If you have had problems getting access to an MS nurse, or have had problems with the service you’ve received, you should read our blog post.
Although Miranda and Lindsay have been named as overall winners, we’d like to reaffirm that, based on the feedback from this year’s campaign, almost all MS specialist are Super Nurses. Congratulations to all of you, and thanks to everyone who has made this year’s ‘My Super Nurse’ such a fantastic success.
Read more about the MS Trust’s work to safeguard the future of MS nurse, and why we’ve focused on fundraising to roll out our innovative tools to help nurses demonstrate the impact of their work.
Spread the word
via My Super Nurse award | MS Awareness Week 2013 | MS Trust supported research projects.
![]()
From the OMS website
Specialist Study Presentation – July 2013
Primary, secondary and tertiary prevention of multiple sclerosis: theory and clinical evidence
In 2012 an Australian research team led by Professor George Jelinek (Founder of Overcoming MS, http://www.overcomingms.org) published research in Neurological Sciences, a major international neurology journal, looking at the health related quality of life outcomes at 1 and 5 years after an intensive MS lifestyle intervention. The evidence presented showed an average of 20% improvement on MS quality of life scores across physical, mental and emotional domains for people with MS following a preventive risk factor modification approach to MS over a 5-year period.
Additionally, Professor Jelinekʼs team has also commenced a major international study of PwMS looking at the various factors in their diets and lifestyles, and their disease activity and disability. This will produce strong evidence about the effect of these factors in MS disease activity and progression. The respondents represent the widest possible range of ages, geographical regions, and with different types of MS. The outcomes of this research will be published in a series of papers during 2013 and Prof. Jelinek will discuss these findings at this seminar.
This presentation will be held on Thursday 4th July 2013 at The Belmont Hotel, De Montfort Street, Leicester, UK.
Following on from my last post about the thinking about viruses as potential drivers of degeneration in MS, here is some initial data from our experiment of using Omegawash as a strong natural detox agent.
At the MS Therapy Centre, Bedford,
12 people have tried taking this strong natural herbal and colloidal detox product, which claims to be anit-viral as well as anti-bacterial. anti-fungal and anti-parasitic. I asked people to fill in the MSQOL 54, a quality of life score with many different elements, both before and after.
Results: 1 person could not take it as it made them feel ill, & 1 for personal reasons; 1 I haven’t managed to follow up yet.
4 people took 1 bottle and did not notice any benefit or change, 2 of them have since had inflammatory activity and viral (coldsores etc) activity.
1 was in a very bad way when took 1 bottle as a ‘last resort’, with continual fatigue & very uncontrolled spasticity; this cleared up, although obviously, not cured of MS and its problems by any means, & MSQOL data has been lost.
4 people took a bottle, felt an improvement in their symptoms, and went on to supplement the 1 bottle funded by the MS Centre with 2 more bottles each.
Because the most noticable theme in people who felt they benefitted was an improvement in energy, this is the item I have looked at first.
Scores on the MSQOL for energy, out of 100, pre and post omegawash, for each of these 4, were:
Before – 4/100 After – 56/100
Before – 24/100 After – 52/100
Before – 0/100 After – 72/100
Before – 48/100 After – 64/100
All of these 4 participants felt that the omegawash had made a significant difference to their energy levels. One of these had also made other changes over the same time period, starting hyperbaric oxygen, and changing her diet.
I have only just started to look at the questionnaire data. I will report on this again once I have chased up my last participant, and looked at the other areas of the MSQOL, and identified any unifying factors in the people who reported benefit.
Today I could say that out of our tiny 10, there was a 10% drop-out rate, 40% no benefit, 10% possible benefit, and 40% reported significant benefits in energy ( and other areas of quality of life which I have yet to analyse). In the ‘responders’ group, there was an average of 39.5 point improvement in energy. Other reported benefits not included in the MSQOL included complete alleviation of bloating and vaginal thrush.
In the interests of science (haha!),’more research is needed’; but in the interests of ‘doing what you can asap as long as it’s not dangerous’, I thought I’d just let you know!
Omegawash is available from www.omegawash.co.uk.
As with all herbal products, you need to check that the ingredients are safe for you to use with your condition and whatever medications you take.
All the best, Miranda
MS Trust conference – part 1.
In November I attended the MS Trust’s annual conference for healthcare professionals working in the field of MS.
I really enjoyed this year’s conference, and will summarise what I learned below.
The first speaker was Gavin Giovanonni, top MS researcher at Royal London Hospital. This is a pic from his blog, which you can follow at http://multiple-sclerosis-research.blogspot.co.uk/ http://multiple-sclerosis-research.blogspot.co.uk/. It includes ‘the mouse doctor’ (?) who is co-blogger.

to this talk resonated with everything I have been thinking for the last few years. You could sum it up as MS – which is more important – inflammation or degeneration? This argument has been recently explored in the article
‘Will the real MS please stand up?’ by Peter K. Stys, Gerald W. Zamponi, Jan van Minnen & Jeroen J. G. Geurts – here’s a link to the full text article http://mssociety.ca/chapters/calgary/pdf/2012_Stys_507.pdf.
This article weighs heavily on the side of looking at the importance of degeneration, so doesn’t really discuss the benefits of early aggressive treatment of inflammation.
Giovannonni’s blog calls this article ‘myopic ramblings’ ; it’s a dog-eat-dog world out there in academia, but Peter Stys has received funding from the MS Society of Canada to research progressive MS, which has got to be good news.
To illustrate what this discussion is about, I’ve done a rough diagram based on one by Professors Coles & Compston Lancet. 2002;359:1221-1231
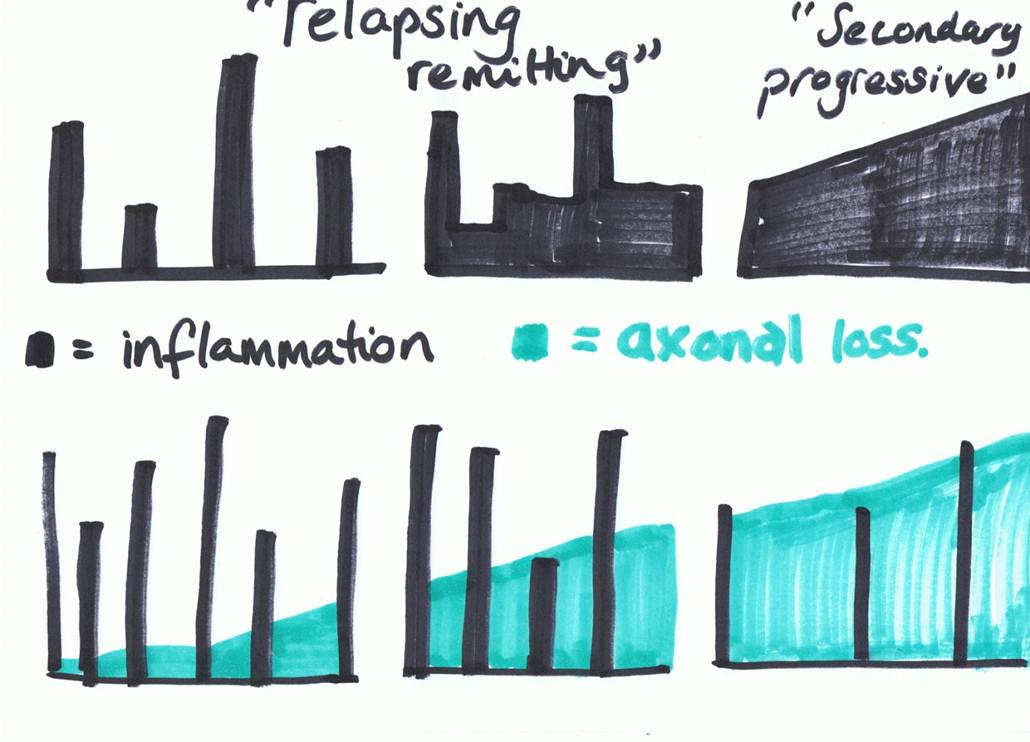
Basically, the tall skyscrapers represent inflammation – relapses or new symptoms. They are the part of MS that pretty much all the research and medications for MS have always been aimed at; that’s why research trials always only want to recruit people with relapsing –remitting MS.
But the disappointment over the last few years has been realising that although the disease modifying MS drugs can show a reduction in relapses, they have not been able to prove a reduction in the progression of MS.
The progressive element of MS is represented by the green block, and represents damage to and loss of axons, the long part of the neurons, or nerve cells.
The argument that Giovannonni presented, which is being mirrored by various thinkers around the world at present, is that perhaps research/pharmaceuticals have been focussing on the wrong part of MS. Perhaps the periods of inflammation in MS are the body’s reaction to a degenerative process that is going on.
As in this article, Giovanonni described his team’s interest in HERVs ( human entero-retrograde viruses – virus which are within the genes) and other virus which we can contract later in life; in particular, the Epstein Barr virus which causes glandular fever, and is part of the Herpes virus family. They want to see whether by suppressing these viruses, the driving force of the degenerative process might be taken out, and they have just received funding to do the preliminary research with anti-virals, which is great news.
It made me think again about looking into powerful natural anit-virals, and I’m going to speak to all the people who tried using some last spring to hear about experiences and see how they’ve been doing since.
Another big factor in his research is Vitamin D; for a long time he has been an advocate of high dose vitamin D3 supplementation. I’ve got previous posts about this so won’t go into the pro side of vitamin D, BUT…

The subject got pretty confusing later when Professor Carolyn Young, Consultant Neurologist and Honorary Professor of Neurology
Walton Centre for Neurology & Neurosurgery, Liverpool led an
Update on Vitamin D.
The professor warned us that this would be a challenging session, and it was. This is really important, as high dose vitamin D has become a mainstay of treatment for anyone who’s had their ear to the ground in the last few years, and neurologists have started to also take it seriously and recommend it.
She introduced us to all the formative research on vitamin D and MS; the Nurse’s study, which is scientifically important and excellent due to the enormous size of the sample – 92,253 women followed from 1980 to 2000) and Nurses’ Health Study II (NHS II; 95,310 women followed from 1991 to 2001. This study showed that having higher vitamin D blood levels, and taking supplements containing vitamin D had a strong effect of protecting a person from developing MS.
The US army study; likewise, great numbers and scope of years, showing 7 million army recruits from 1992-2004 and compared the vitamin D levels with their risk of developing MS.18 They found 257 new cases of MS in the group. There was a significant decrease in risk with increasing vitamin D levels among white, but not black or Hispanic people, who had lower vitamin D levels than whites. Levels of around 100nmol/L or more seemed to be protective, with almost a two thirds reduction in risk for those with these higher levels.
A good factsheet summarising research on vitamin D and MS is on the MS Trust website at http://www.mstrust.org.uk/downloads/vitamind.pdf
She then gave feedback on 4 or 5 more recent studies, where vitamin D supplementation ( mostly D3 but one study used D2) was given at various doses, over various timescales, none of which showed any influence on annual relapse rate, or level of disability at all.
We then went on to discuss what to make of this?
One point was that an association is not necessarily a cause
For example, low levels of vitamin D in the blood are associated with relapses in MS – but maybe they do not go towards causing it – maybe the low level of vitamin D is caused by the relapse or inflammation?
One point was that it may not be possible to extract the active ingredient – whatever that is – from the foods in order to make an effective supplement, and that sometimes other helpful substances in foods are responsible for the absorption of a nutrient.
I asked whether there was a difference between getting your vitamin D from the action of sunlight on the skin and a supplement? I didn’t get the full answer I was looking for, but Prof Young did make the point that there are other actions that the sun has on the immune system and inflammation that are generally beneficial.
People wanted to know what we should advise ‘while the scientists work it out’. Prof Young’s advice was that she felt that 1000IU should be the top recommendation a healthcare professional makes to a person with MS, and that it chould be checked that the person doesn’t have any kidney problems, as if they do, high dose vit D could cause kidney stones.
I’m going to ask Giovannonni on his blog/twitter/whatever what his response to this is, and also check what George Jelinek has been making of it.
I think if I have any thoughts on this so far, they are that perhaps people with MS need to try to get a s much Vit D as possible from foods and from the action of sunlight on the skin. In this country that only works between April and October, and when the sun is high in the sky.
It makes me wonder about sunbeds, I haven’t gone right into this, but just asking around, apparently you can get vitamin d from using a sunbed, but it has to put out UVB rays.
( and obviously, use sensibly, don’t get burned or overdo it)
I think I’m probably going to carry on recommending 5000IU, due to all the other research I’ve seen, but will be keeping my ear to the ground.
I’ve got more from the conference and will post as soon as I get time to write it up!
We also had a great time at the gala dinner fancy dress night, so In the meantime, this is for the Bedfordshire people – if you ever wondered whether your MS nurses were arch rivals or accomplices in crime, here’s something to confuse you further….!

haha
it’s not my normal look…
but I did enjoy being Marylin for the night!
Muscle stiffness and spasm (2) Hi, can’t beleive it’s November already! I’ve been busy making presentations that I’m now going to try to post up here. This one is about muscle spasm and stiffness. It’s a powerpoint, so we’ll see if it works!
Yay! Ok, so if you click on the link, you can download the powerpoint.



