2012
Supplements
The Therapy Centre is going to stock the supplements that I recommend most, at a discount of 15% off the RRP (which is fantastic news). So soon you will be able to buy Vitamin D3 5000 IUs, cold pressed flax seed oil 1000mg (Omega 3), and 2 varieties of an iron-free multi vitamin, mineral and nutrient supplement made from whole foods. I got mixed up with a discount code previously, so if anyone used it and didn’t get the 20% discount, massive apologies, it went direct to the Centre, if you want to claim it back, see me!
Food
For people who’re eating food without saturated fat, but struggling with what to eat, I found a great website, www.fatfreevegan.com. Also, the OMS site is collecting more recipes that you can see when you log in. I too am collecting recipes, tips and ideas, so anyone out who has some good ones, please email or bring them in!
Hot topics
A hot topic for me this past year has been Epstein Barr (glandular fever) virus and herpes virus (mainly herpes, cold sores and shingles in adults). Since I started asking people if they had these viruses, I’ve been shocked at how many MS people have one of these. Recent research showing Epstein Barr still alive in MS lesions at post mortem, and discussion around the fact that the virus lives on and may drive inflammatory processes, got me wondering whether there could be a natural or herbal way of killing off the virus, and whether this would have any effect on the MS. So watch this space for the results of this latest quest – natural viral detox!
Got a great tip the other day – did you know that the Kindle (£150 version) can read your books to you? And for some people with vision problems, the iPad is a revelation, so keep your eye on how technology can make life easier!
*******************
December 2011
As an MS Nurse, I’m always looking for the best advice to give to my clients about being and stayingwell….. MS is a disease with a genetic component, but our environment – the food we eat, the climate, exposure to various viruses, and stress, – have an impact on activating or suppressing our genetic susceptibilities. I often talk with people about their lifestyle and diet, and depending on what I find out, I may recommend that they look at the work of Terry Wahls, Ashton Embrey, Ann Boroch or Sawyer & Bachrach , or get an overview and understanding of the different considerations and approaches by reading Judy Graham’s book.
But at the moment, if I had to choose just one piece of advice to give to people with MS who want to know what they can do to help their health, it would be to go to the http://www.overcomingms.org/website, and immerse themselves in the evidence based information there.
George Jelinek is the author of the book and website ‘OvercomingMS’ . He is a medical doctor, and professor of emergency medicine in Australia, whose mother had MS and became very disabled, and who was diagnosed himself in 1999. Since that time, he invested a vast amount of time and energy into examining the research on the various dietary, nutritional and lifestyle factors that have a documented effect on MS, found evidence of the profound difference they can make, put the recommendations into practice and stayed symptom and relapse free, and has put this together into a simple to follow approach.
The work that Professor Jelinek has done in compiling and explaining, in simple language, the research on dietary fats and vitamin D is incredibly helpful, and the fact that it’s all in one place, on the web or in his book,
Overcoming MS, an Evidence Based Guide to Recovery’ means that the information stays cohesive and doesn’t become overwhelming
The cornerstones of the OMS approach are:
Diet and supplements
· Omega-3 fatty acid: 20g /mls a day of flaxseed oil or fish oil, or the equivalent amount of fish
· Optional B group vitamins or B12 supplement if needed
Meditation – 30 minutes daily
Vitamin D
Sunlight 15 minutes daily 3-5 times a week as close to all over as practical
Vitamin D3 supplement of at least 5 000IU daily, adjusted to blood level
Aim to keep blood level of vitamin D high, that is between150-225nmol/L (may require up to 10 000IU daily)
Exercise – 20-30 minutes around 5 times a week preferably outdoors
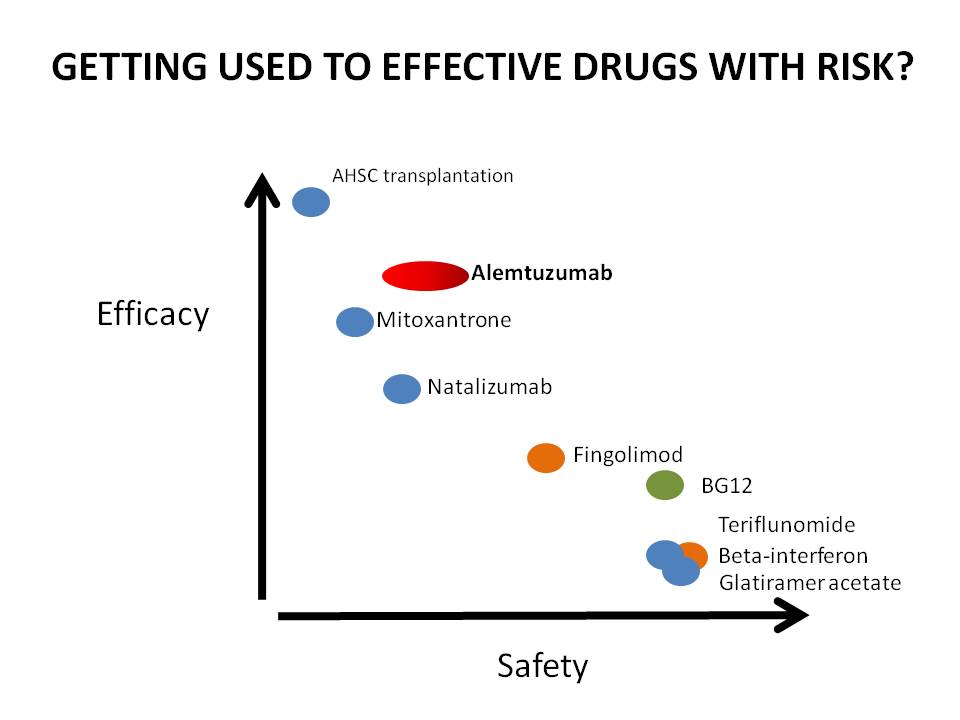
Medication
· In consultation with your doctor, if a wait and see approach is not
appropriate, take one of the disease-modifying drugs (many may not need
a drug, and drug selection should be carefully weighed against side effects)
· Steroids for any acute relapse that is distressing
· One of the more potent drugs if the disease is rapidly progressive
The down side to the evidence-based approach, is that if anything – be it a therapy, foodstuff, supplement, drug, or approach, has not been researched, or not researched to an adequate standard, then it can’t be counted. The evidence based approach prevents us from wasting money or time on useless therapies, but as Carl Sagan, famous America
astronomer, writer and scientist, famously said, ‘absence of evidence is not evidence of absence’. So I’m still happy to suggest a person, for example, who has extreme fatigue, might try Terry Wahl’s green smoothies, or that someone might try hyperbaric oxygen, or even some of the commonly used symptom management drugs ( for instance for muscle spasm and stiffness) which don’t necessarily have a body of scientific evidence for effectiveness behind them, but are used due to the effects that people report.
Recently I was really excited to see a research paper from the Australian Journal ‘Quality in Primary Care’, following up people who attended an OMS retreat and took on the recommended dietary and lifestyle changes. This study showed ‘ongoing improvements in health related quality of life after an intensive lifestyle modification course’, over 2 ½ years, that ‘ could potentially make a significant difference to the lives of many people with this condition’, and ‘contribute to the growing body of evidence that health promotion programmes and non-drug therapies for MS patients have a beneficial effect.’
We hope to get Professor Jelinek over to the UK for a retreat in summer 2013, but you don’t need to do a retreat to take on this approach –all the research and recommendations are outlined on the website and in his book. Recently I met up with Lisa, the moderator from the website, and two English women who have done the OMS retreat, follow its recommendations, and enjoy good health, and introduced them to the MS Trust. Now they are going to be introducing the work to the MS specialist practitioners at the annual MS Trust conference for healthcare professionals in November. The goal of this is to help to promote the work of OMS in the UK – so that everyone who gets diagnosed with MS has the chance to find out about it, research it for themselves, and make their own decision.
************************
spring 2011
This month I am mainly focussing on Urinary tract Infections (UTIs), because they can really set you back when you have MS, and Prevention is better than cure!One cause of UTIs with MS is the bladder not emptying properly. Not being able to start passing urine, feeling there’s some left afterwards, passing a fair amount again quite soon after, ‘urgency’ and UTIs can all be signs of incomplete emptying. This needs to be identified by ultrasound scan, which is done during an assessment by the continence service. For Bedfordshire, Melanie runs a clinic here once a month, or for Beds and Northants you can be seen in a local clinic , or have a home visit. Speak to me, a nurse or your GP to be referred
Be prepared! Burning, cloudiness or unusual smelling urine are classic signs of a UTI, but you can also dipstick test your urine at home. Buy Multistix or Uristix which include Leukocytes and nitrites,.Also dipstick if you have a relapse, as UTIs can be symptom free. It’s a good idea to help your GP understand how a UTI can cause MS to flare up, and be ready to prescribe an antibiotic at the first sign of infection. Get a sample taken in too, and the antibiotic can be changed lagter if necessary.
If you use a catheter, either a permanent or intermittent type, this also can introduce a route for infection. Obviously scrupulous hygiene is a must. People who get recurrent infections can try having antibiotics for the three days around a catheter change, or may even need to use a daily low dose antibiotic. For intermittent catheters, the type can make a difference – it’s important to use something that you don’t have to touch the tip of at all, and there are a couple out now which have a protective ‘introducer’( Hollister ‘Vapro’ is one), so the tip does not even touch the outer part of the urethra. Talk to your continence adviser.
if you get a UTI.
Don’t take any chances – Get a prescription of antibiotics! If you take a course, top up with probiotics during and afterwards to help protect your digestion and health. Always finish a prescribed course of antibiotics, as stopping early can cause antibiotic resistant bugs.
Drink plenty of water and pee frequently. Begin as soon as you feel the first signs and symptoms. Doing this can actually flush the bacteria out and wash it away. Avoid alcohol, caffeine, fizzy drinks, spicy foods, and bubble baths etc, which can worsen symptoms. Cut out sugar to help your immune system fight back.
The most common bug causing UTIs is E coli, which lives in the bowel, but can cause persistent problems once it enters the urinary tract. So – what else can you do to help get rid of RECURRENT UTIs, especially if antibiotics are not working?
You may want to consider using Colloidal Silver – silver particles suspended in water, which is a natural antibiotic. Go to http://www.ukcolloidalsilver.co.uk/
“Citricidal’ from Higher Nature is a safe, natural antibiotic you can try at home.
Cranberry helps to acidify urine, and may help stop the bacteria form sticking to the bladder walls. Concentrated tablet form is best.
Some people have found D-Mannose to be effective in the same way – this is a simple sugar that E coli tends to latch on to. It’s available online but is quite expensive.
All these remedies can be taken both in a higher dose for infection, and at a low dose as a preventative.
Be aware:
· Some sexually transmitted diseases have symptoms similar to urinary tract infections. See a doctor if you suspect that you may have an STD.
· See a doctor if you have a fever, chills, pain in the flank area, nausea or vomiting – especially if the symptoms develop rapidly. Also see a doctor if symptoms do not improve after 24 hours of self-care, or if you are unable to urinate at all.
*********************
December 2010
I hope everyone is reading the MS Resource Centre’s New Pathways (available to read at the MS Centre) at this exciting time in the world of MS treatments. The July/August edition updates us on the CCSVI debate, and lists all the places worldwide where you can be screened and treated. To learn more, I am attending the first International conference on CSSVI in Glasgow, in October, so I’ll be sure to report back.
The same New Pathways reports on a couple of fascinating small studies which fit in with this theory of poor circulation from the brain, and have worked for most of the people on the trial.
Inclined Bed Therapy
This involves raising the head of your bed by 6 inches. It’s certainly a lot cheaper than a private operation in Poland, as bed raisers, risers, or ‘elephant feet’ can be bought online for 12.99. Since CSSVI hit the headlines, this research has attracted fresh attention, and the author is carrying out a larger survey. You can get involved by going to www.thisisms.com/ftopicp-118378.html#118378
Update on Vitamin D
Thank you to the lady who came to let me know that she’s been feeling much better since she started on it. It is always good to get feedback; good or bad! D3 is still coming up as good, but newest research suggests it’s not just the vitamin D component that’s so important, it’s also the ultraviolet light, so more reasons to get outside as much as possible. Had a good question regarding the vitamin D Should you take CALCIUM with it? I discussed this with the technical advisers at Nutri, who supply quality supplements to practitioners. Their view was YES, if you are on a dairy free diet, but not if not. Also, if you quote MSRC New Pathways when you make an order on the phone at NutriCentre, you get 20% off.
My little break from clinic afforded me some reading time, and I’ve just finished ‘Healing Multiple Sclerosis’ by Ann Boroch. I’d recommend this to anyone who has taken lots of antibiotics in their life before having MS, or has had recurrent yeast or fungal infections (like thrush or athlete’s foot) It’s main drive is about the association between chronic candida and MS; this isn’t a new theory, and most natural health practitioners understand all about it. Getting rid of candida overgrowth is a long slog, but worth it if it applies to you, and I’m also happy to help anyone with this 3 pronged attack – kill yeast, don’t feed yeast, put good bacteria back! The author’s attitude to illness is a bit over the top at times, but the candida bit is good.
MS Centre Dietitian Bernice Chiswell adds
‘However, it should be born in mind that there is no scientific evidence behind this. The diet is very restrictive and for the majority could prove more harmful than beneficial due to inadequate macro and micro nutrient intake’
Me: The next book was ‘The MS Recovery diet’ The theory behind this is that food intolerances can initiate inflammatory reactions in the body, and it makes excellent and logical reading. It’s a similar approach to the Best Bet diet, but assumes that your intolerances are likely to be individual, explains how to find out, and has a large recipe selection to help get started. I recommend this to anyone with MS in the family.
Bernice Chiswell adds;
‘It should be born in mind that, although people with MS can have food intolerances, the only sure way to test for this is by food exclusion and re introduction. Again, unnecessary exclusion can lead to unbalanced diets, plus be an added life burden to people who are already coping with disability and fatigue. The best bet diet is again not evidenced base.’
Me: It’s a great month for books, too, as 3 new publications are out which all deserve reading – I have been waiting for ages for 2 of them:
Terry Wahls’ ‘Minding my mitochondria – How I Overcame Secondary Progressive MS and Got Out of my Wheelchair’, which promises to be very scientific and convince everyone to eat loads of greens; ‘Overcoming Multiple Sclerosis; An Evidenced Guide To Recovery’ by George Jelinek. Check out his approach on his website of the same name. Basically, super low fat Swank diet, a disease modifying drug and meditation, and Judy Graham’s ‘Managing Multiple Sclerosis Naturally’. I haven’t read these yet but I will be doing and will report back!
Dietary approaches vary a bit, but some things remain constant – the less saturated fat, and the more brightly coloured veg & omega 3 fatty acids you eat, the more good you’ll be doing yourself.
Remember, if you’re taking something out of your diet, make sure you balance your nutritional needs. Our expert dietician, Bernice, can advise you.